News Story
Resident Doctors' Day & I am a Doctor

Stay updated with the latest news, updates, and media releases from NZRDA.
Filter by category
News Story
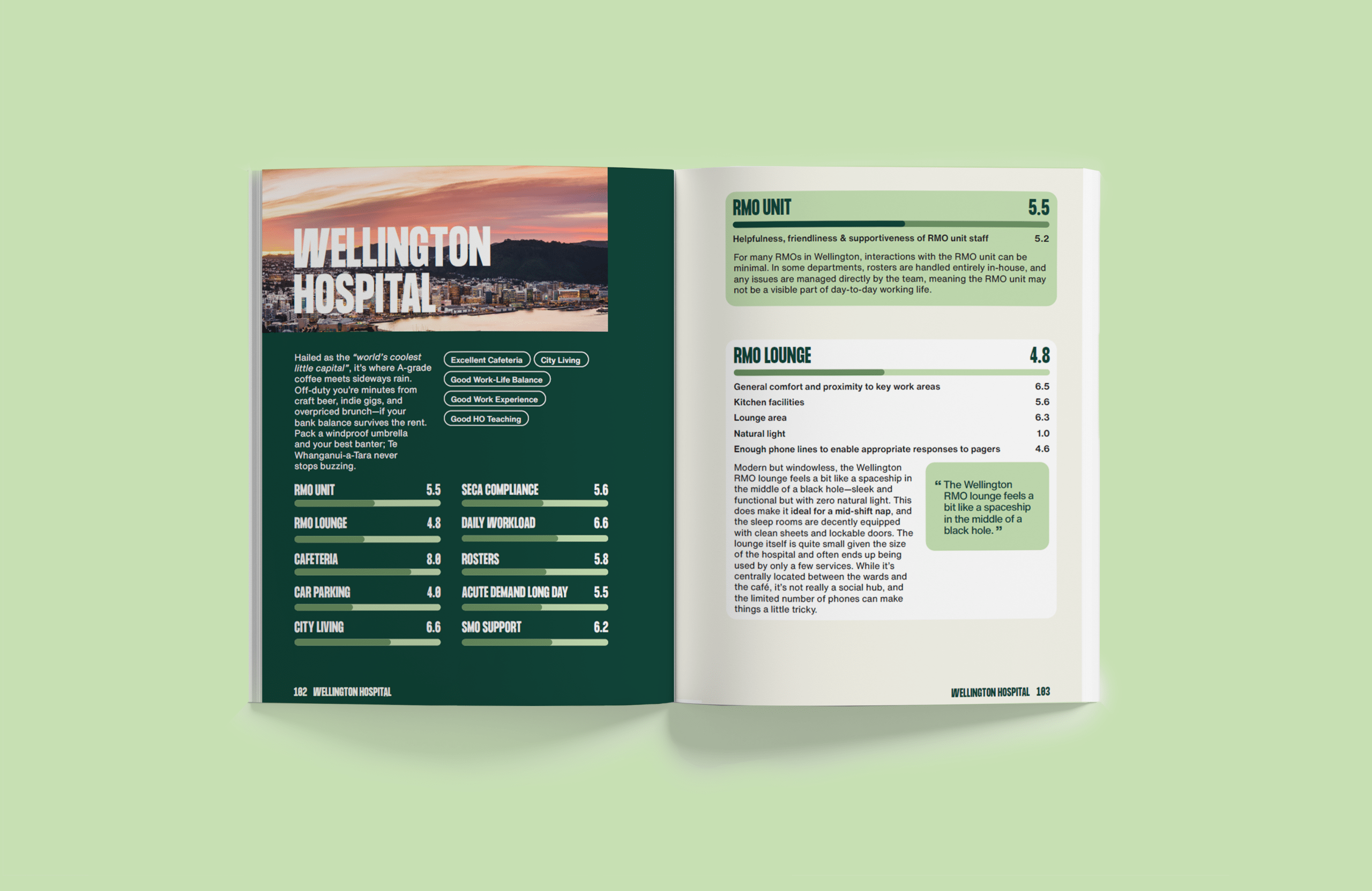
Publication
News Story

Opinion Piece
Opinion Piece
Opinion Piece
News Story

News Story
News Story
Media Release
Media Release
Publication
